Epigraph Vol. 21 Issue 2, Spring 2019
Success after surgery: What is it and who decides
What does “success” look like after epilepsy surgery? Though the common perception is that success equals seizure freedom, the full picture is more complex.
For people with drug-resistant epilepsy, surgery does offer the potential for a cure. In children and adults undergoing temporal surgery, short-term rates of seizure freedom have been reported between 67% and 85%, with 10-year rates estimated between 50% and 55%. In children undergoing multilobar or hemispheric surgeries, seizure-free rates can reach 80%. Seizure freedom can be life altering for patients and their families.
But even when seizure freedom is achieved, the consequences of the surgery and removal of part of the brain can affect quality of life. These consequences—particularly the emotional and social ones are sometimes downplayed or dismissed, yet they can limit a person’s quality of life as much as persistent seizures can.
What makes for a good quality of life?

Though most studies find that quality of life does improve markedly after epilepsy surgery, emotional and social functioning appear to be more dependent on factors such as age at the time of operation, sex, age at diagnosis, educational level, and squishier personality-related factors that haven’t yet been well defined.
In addition, someone’s interpretation of what constitutes a “good quality of life” may change after successful surgery.
“It's not just down to seizure freedom or not,” said Sally Baxendale, consultant neuropsychologist at the UK National Hospital for Neurology and the University College London’s Institute of Neurology. “We need better measures and predictors of outcomes, which we don’t have.”
Cognitive impairment
A serious consequence of epilepsy surgery is cognitive impairment, said Barbara Jobst, the Louis and Frank Ruth Professor of Neurology at Dartmouth’s Geisel School of Medicine and head of the Dartmouth-Hitchcock Epilepsy Center, USA. “Unfortunately, we often kind of ignore that fact.”

Existing studies following patients after temporal lobe surgery tend to see cognitive declines in the first two years, followed by stability in patients who have achieved seizure freedom. A 2018 study found that memory could actually improve years after surgery, particularly in patients who were seizure free and reduced their use of anti-epileptic drugs.
In some cases after surgery, people continue to have seizures while also experiencing serious cognitive issues, said Baxendale. “They’ve paid a heavy price and they aren’t seizure free; they’re in the worst of all worlds,” she said.
The persistence of seizures is not an overall mark of failure, she noted. “If patients still have seizures but no longer are having disabling seizures, or if they’re no longer doing some embarrassing thing that they used to do –spitting, hurting themselves, undressing, all sorts of things – they may be happy with that outcome,” she said.
Even when seizures are reduced but not eliminated, most patients do not regret having surgery and say that it has improved their lives.
Psychological issues: Present and persistent
However, beyond seizure frequency and cognitive issues lie psychosocial and emotional issues that sometimes go unaddressed.
Depression is a risk factor after any major surgery; it also has a complicated relationship with cognitive decline, as each condition puts the person at risk for the other. For people with epilepsy, depression and anxiety can affect their post-surgery quality of life, even if their seizures have stopped.
The strongest risk factor for depression after surgery is depression before surgery, though post-surgery depression can arise de novo in anywhere from 5% to 25% of patients. A study of 253 patients with long-term follow-up (mean 10.6 years post-surgery) found that antidepressant use had increased from before surgery (from 22% of patients to 30%); however, 92% of patients considered their surgery worthwhile.
Other risk factors for post-surgery depression include older age, male gender, a family history of psychiatric illness, and lack of seizure freedom.
Anxiety can arise after surgery in between 3% and 26% of patients. Psychogenic non-epileptic seizures also can appear in about 4% of patients. In females with a history of psychological issues, the incidence is closer to 9%.
As a group, people with epilepsy are at an increased risk for suicide, somewhere between 2.5 and 5 times that of the general population. Though few studies exist, the research literature suggests that risk does not seem to decrease after surgery—even when seizure freedom is achieved. A 2011 prospective study found a suicide rate 3.4 times that of the general population in adults five years after surgery.
Experts suggest that psychological issues should be addressed via:
- A thorough psychological assessment and diagnosis before surgery, including a family history
- Counseling of patients about the biological and psychosocial factors involved in the development of depression after surgery
- Psychological support before and after surgery
The reality is, said Baxendale, “Very few epilepsy centers have the appropriate support systems to help people work through these psychosocial and emotional issues. Having psychologists and other counselors who are dedicated to people with epilepsy doesn’t really exist.”
Burden of normality
A small percentage of people will be seizure-free with minimal measureable consequences to the surgery, but have problems adjusting to the changes. The “burden of normality" can stress relationships and disrupt the lives of the person with epilepsy and those around them (particularly spouses and caregivers).
As noted in a recent review, “Seizure relief may decrease dependency and the level of consideration displayed by others, and increase expectations toward the now ‘cured’ patient. This may … cause depression and anxiety and may destabilize a relationship that was predicated on one party being dependent on the other.”
The expectations of seizure freedom as a gateway to employment aren’t always borne out; the best employment outcomes appear to be in people who were seizure free after surgery and who were already employed, or were students, before surgery. Employment rates may decline after surgery, even if more people gain the ability to drive. A 2018 study found that after surgery, employment remained unchanged or declined in 22% of patients; employment status improved in only 3%.
One study of people who had extratemporal surgery found a 43% seizure-free rate (Engel class IA) but did not see a corresponding rise in employment rate. The study did find that seizure freedom led to people working more hours and taking on more demanding jobs, but such changes also occurred—though less frequently—in people who were not seizure free after surgery. However, seizure freedom was associated with driving, having a partner, and lower scores on a depression inventory.
While surgery has been shown to be effective in older people—including those aged 60 and older—Baxendale said the consequences of successful surgery can be particularly difficult to handle in this group. “If they have had a long history of seizures, they haven’t really been able to grow up – they don’t have the education or employment,” she said. “And then they’re pushed out into the world without skills or experience.” There are some studies that suggest that integration following surgery is easier for those who worked and were active before surgery, in comparison to people who were more isolated.
Jobst noted that in Germany, patients can undergo a month-long rehabilitation program after epilepsy surgery that focuses on psychosocial factors—driving, employment, relationships—and adapting to life with no seizures, or with fewer seizures. Some of these people have been disabled most of their lives, she noted; “They may have anxiety or problems adjusting to a fairly normal life. These programs can lead to better outcomes.”
Pediatric epilepsy surgery
Pediatric issues after surgery can be more complex, because children with epilepsy may be faced with more extensive surgery, such as hemispherectomy/otomy or corpus callosotomy. These procedures can stop seizures between 50% and 80% of the time—but they have multiple and sometimes lifelong consequences.

“For a very large population of children who have intractable epilepsy, surgery is a terrific solution,” said Monika Jones, co-founder and CEO of the Brain Recovery Project. “However, what is not always discussed is the broad range of functional outcomes you can have after some of these bigger surgeries, and what to do about it.”
Jones’ son Henry had three surgeries when he was only a few months old. “He had to have the surgery, or he was going to die,” she said. Now, Henry doesn’t speak and is profoundly intellectually impaired. “And he can hardly walk,” said Jones. “Nobody wants that story. I don’t regret the surgery, but I wish I had known that all of these challenges would come, rather than having to figure it out along the way.”
As a result of their experience, Jones and her husband Brad established the Brain Recovery Project, a U.S.-based nonprofit that funds new research and provides information and resources to families facing pediatric epilepsy surgery. It also manages a global patient registry designed to gather information to help clarify and understand the developmental trajectory after epilepsy surgery.
Multiple consequences
While parents are informed of near-term risks and consequences, they can be left unprepared to navigate the medical and educational systems for years to come in order to get services and help for their child. Jones would like to see families supported by a team of professionals after surgery, including a neuro-ophthalmologist, audiologist, physical therapist and others, to help with the many areas of surgical consequence that are often not discussed before the operation. Some of the common and predictable consequences of the surgery include visual field loss, auditory processing, impaired reading ability, hydrocephalus and endocrine and development problems.
Many parents misunderstand the extent of vision issues after surgery, believing their child will have only peripheral vision loss. However, children can experience the loss of the entire visual field opposite the removed hemisphere (homonymous hemianopsia). “That can have a tremendous impact on a child,” noted Jones, including difficulties in learning to read. “It becomes much more challenging if you can see only half a letter, or half a word.”
In addition, many children may have auditory processing issues after hemispherectomy, because the auditory cortex is removed or disconnected. These issues can have a profound effect on learning and social interaction.
Reading after a major surgery can also be a problem. One of the few recent studies on functional outcomes after hemispherectomy found that only 42% of children aged 6 and older had satisfactory reading skills. Only 6% of school-aged children were in mainstream schools without additional educational support; 59% received educational support in mainstream schools and the other 35% were in special schools or cared for at home.
A 2015 review found hydrocephalus rates of 14% up to 1 year after surgery, but Jones has heard from patients and families that hydrocephalus can cause concern throughout the lifepsan. “People who have had surgery as children sometimes report severe headaches, hydrocephalus or other complications in adulthood,” she noted. “But if they are seizure free after surgery, they’re usually released from care after a few years. So if things happen down the road and you don’t have a neurologist, then the neurologist you do see doesn’t know what to do.”
Some issues can appear months or years after a surgery. Though there’s a lack of published research, some families report neuroendocrine challenges after hemispherectomy, such as precocious puberty or adrenarche, growth issues, diabetes and weight gain.
More knowledge, more guidance
A lifetime of consequences is difficult to convey in a few conversations with a neurosurgeon—but the system makes it easy for parents to be lost between the surgery and its fallout, said Jones. In many cases, there is little to no support post-surgery—especially if the seizures stop and the surgery is deemed a success.
“Can you imagine having a knee replacement and your doctor saying, ‘So hey, I replaced your knee, good luck – get a lot of therapy! You can stand right now so you’re good’ – and that being all?” said Jones. “Isn’t the right answer to say, ‘Look, this is going to stop the seizures, but these are the challenges your child is going to have’, and provide guidance?”
After 12 years as an advocate, Jones’ position is clear. “Very few parents regret a hemispherectomy but most of the ones I have talked to wish they had known more, and had guidance. That’s all we want.”
A successful surgery for epilepsy can have a positive impact on a person’s life. However, the consequences of surgery extend beyond a simple seizure count. Some of these consequences can be at least as limiting as the seizures themselves. Clinicians who see these long-term effects agree that we need to do a better job of advising patients about all the potential consequences, so that they recognize these issues if and when they arise.
Appropriate support services also are necessary to help patients and their families manage these aftereffects. Most programs do not have these services and may not yet recognize the full spectrum of consequences of epilepsy surgery.
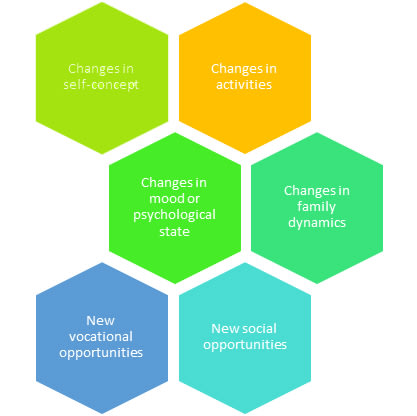
Features of the “burden of normality” that can affect quality of life after epilepsy surgery. Adapted from Wilson, S. J., et al. 2007. Epilepsia, 48: 13-16. doi:10.1111/j.1528-1167.2007.01393.x
Subscribe to the ILAE Newsletter
To subscribe, please click on the button below.
Please send me information about ILAE activities and other
information of interest to the epilepsy community