Epigraph Vol. 20 Issue 2, Fall 2018
Neonatal seizures: Closing the knowledge and treatment gap
Update: In February 2021, the ILAE Task Force on Neonatal Seizures published a modification of the 2017 ILAE Classification of Seizures and Epilepsies that is specific to neonates: The ILAE classification of seizures and the epilepsies: Modification for seizures in the neonate
Seizures are more common during the neonatal period than any other time in life, occurring in 2 to 3 neonates per 1,000. Incidence is even higher in preterm infants, with some studies finding rates of up to 130 per 1,000.

Despite their frequency, the topic as a focus of research “is so neglected,” said Ronit Pressler, UCL Institute of Child Health & Great Ormond Street Hospital, UK. Pressler gave a presentation on neonatal seizures as part of the Chairs’ Symposium at the 13th European Congress on Epileptology (Aug. 26-30) in Vienna.
Most neonatal seizures occur during the first 24 hours after birth, and are most often caused by something other than epilepsy. The most common cause is hypoxia, a loss of the oxygen supply to the brain. In premature infants, the seizures are often due to cerebrovascular hemorrhage or infarction. Other causes include brain malformations, infections, genetic syndromes and metabolic issues.
The cause of the seizures determines the prognosis, as well as the treatment strategy.
Diagnosis requires EEG
Diagnosis is difficult due to the seizures’ subtlety, Pressler said. Some normal infant movements may be misdiagnosed as seizures, while some seizures are overlooked as normal movements. As a result, using only clinical observations to diagnose neonatal seizures may be no more accurate than a coin flip.
Pressler reviewed a 2009 study that asked 137 health professionals (91 physicians, 46 others) to evaluate 20 video clips of neonates for seizures. (Eleven of the 20 were having seizures.) The average percentage of correct diagnoses was 50%, and physicians were no more accurate than other health care professionals.
To further complicate the picture, more than half of neonatal seizures are clinically invisible, seen only on EEG. Because of this phenomenon, the generally accepted definition of a neonatal seizure refers to abnormal EEG activity, rather than clinical signs.
Because the excitatory and inhibitory neurotransmitter systems are not fully developed, the neonatal brain is relatively prone to seizures. In the past, said Pressler, it was thought that the still-developing brain also was more resilient; as a result, neonatal seizures were not viewed with much concern. But research has shown that seizing neonates are at higher risk for death, as well as later developmental delays, cerebral palsy and post-neonatal epilepsy.
Etiology of Neonatal Seizures

Open treatment questions
Given that seizures usually indicate an underlying, serious issue—“These babies are already critically ill,” said Pressler—it’s still not clear which long-term complications result from the seizures themselves and which stem from the underlying cause. Still, there’s general agreement that neonatal seizures should be treated promptly and aggressively; how to do that is an open question
Only one drug—phenobarbital—is approved for treating neonatal seizures. Effective in only 30% to 40% of cases, the drug may extinguish the clinical signs of seizures but not the electrographic ones (visible on EEG), a phenomenon known as uncoupling.
“Phenobarbital has been used for seizures for the past 100 years,” Pressler noted. “It’s hardly used for adults and older children anymore because of its side effects. But it’s so difficult to do drug trials in babies, which is why no other drug has been approved so far.”
Neonatal status epilepticus
Because neonates tend to have short-lived seizures—most are under 2 minutes—there’s also no good data on what constitutes neonatal status epilepticus (SE). “A seizure over 2 minutes is definitely not good,” said Pressler. “But there are no guidelines on when to start treatment [for SE], and without a definition that all doctors use, it will not be treated.”
Pressler cited three variations on the definition of neonatal SE, culled from published studies:
- Continuous seizures for at least 30 minutes, or recurrent seizures over at least 30 minutes without a return to baseline neurological activity
- Seizure activity for at least 30 minutes of an arbitrarily defined 1-hour time period
- Electrographic seizure activity that occurs for more than 50% of the recording time (usually 30 minutes)
Based on these definitions, said Pressler, between 10% and 30% of babies with seizures experience neonatal SE. But studies have found an increased risk for poor outcome above a lower threshold of 12 to 13 minutes of seizure activity per hour.
Though new treatment options are limited, increasing adherence to current treatment standards can improve outcomes. A 2016 study followed the implementation of a standardized protocol for neonatal SE at the Riley Hospital for Children, Indianapolis. The 12-month project led to several improvements:
- Reduced progression to neonatal SE (46% to 36%)
- Decreased maximum concentrations of phenobarbital (56.8 ug/ml to 41.0 ug/ml)
- Decreased length of stay by 9.7 days
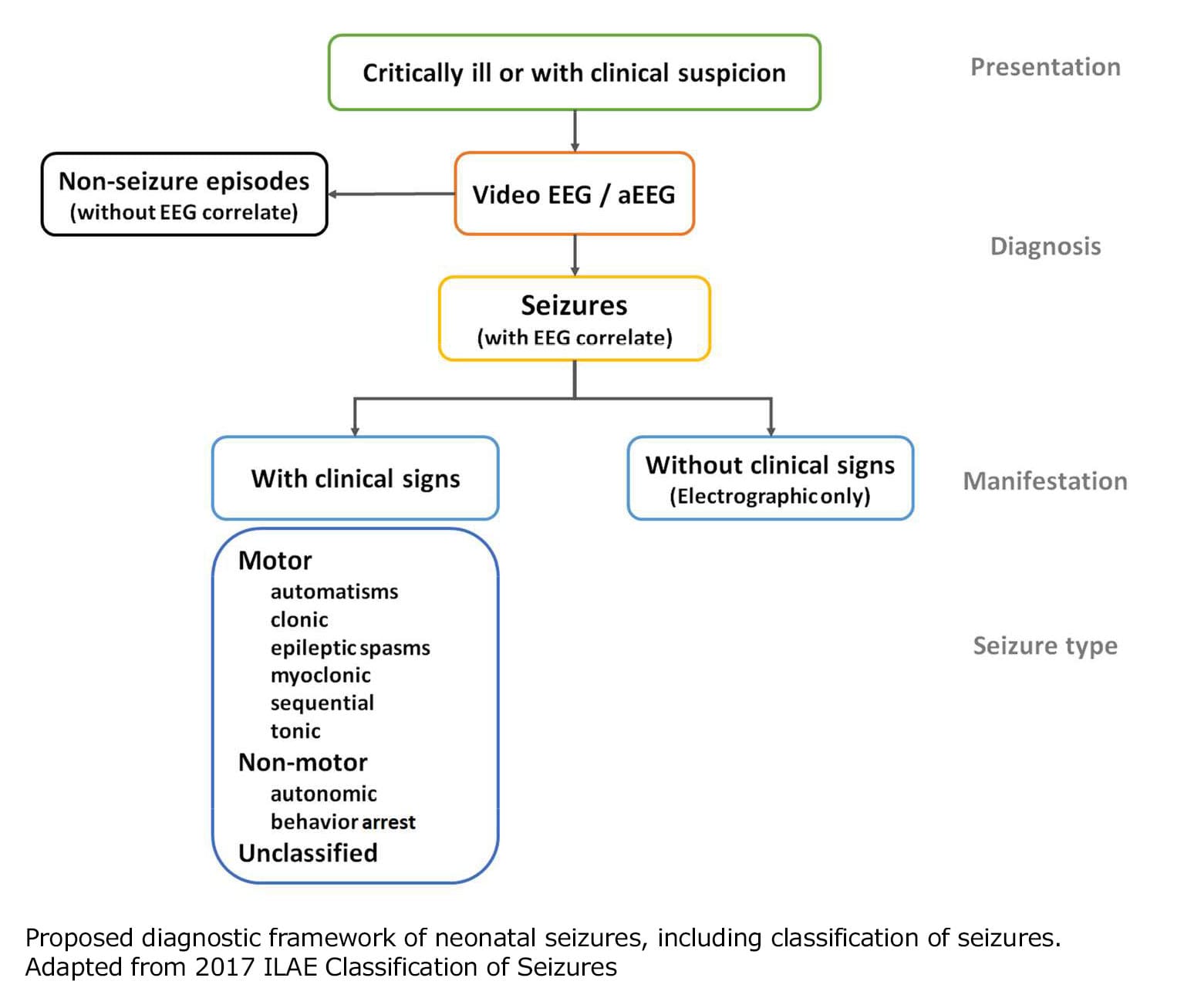
Proposed neonatal seizure classification
The ILAE task force’s proposed neonatal classification framework emphasizes the role of EEG in the diagnosis of seizures in the neonate and includes a classification of seizure types relevant to this age group. Pressler and her colleagues hope that the classification system will lead to improved awareness of the diversity in the causes of neonatal seizures, which may, in turn, lead to more tailored treatments and improved long-term outcomes.
Subscribe to the ILAE Newsletter
To subscribe, please click on the button below.
Please send me information about ILAE activities and other
information of interest to the epilepsy community