Epigraph Vol. 17 Issue 1, 2015
Preventing Death in Epilepsy

It is well recognized that people with epilepsy have a much greater morality rate than the general population. In recent years Sudden Unexpected Death in Epilepsy (SUDEP) has received much, and appropriate, attention, but its causes and a solution for this great tragedy remain elusive. However, there are a number of other reasons for the increased risk of death among those who suffer from the disease, and many of these causes can be reduced or eliminated. At the European Epilepsy Congress in Stockholm, Professor Torbjörn Tomson of the Karolinska Institute reviewed these other causes and some of the measures that might be taken.
In epilepsy there are many contributors to higher mortality. In some cases, the underlying cause of the epilepsy is progressive and fatal and in other cases, while rare, the treatment itself, often from a drug reaction results in an early death. However, it is the epilepsy and seizures themselves which contribute the greatest to the increased number of premature deaths. Although SUDEP is the cause that attracts the greatest attention, especially in western countries, in other parts of the world injuries sustained during a seizure are a major and at times overwhelming contributor to epilepsy related mortality. Status Epilepticus, especially in regions with poor emergency services, can also be a major cause. Suicide, on the other hand, is an often underestimated or unrecognized cause of death in people with epilepsy and is no doubt associated with the high prevalence of depression among these individuals.
One of the important points that Dr Tomson made was that the mortality varied greatly across countries and that the causes of death were different and related to the conditions in each country. For example, in rural China drowning is the overwhelming primary cause of death (about 45% of all epilepsy-related deaths) among people with epilepsy, whereas in Kenya Status Epilepticus caused almost 40% of all epilepsy associated deaths (Figure 1).

Figure 1. Causes of epilepsy-related deaths in four different countries. The figure emphasizes the issues that need to be addressed to reduce mortalities vary across cultures and resources. Of note, in Sweden, the risks also shift with age, with suicide being a leading cause among younger patients.
Although the data don't exist for many countries, suicide is a significant contributor as well, and numerous studies have the consistent finding that the risk for suicide is well above the rate found in the general population (Figure 2). These observations emphasize that, with proper interventions and precautions (and, in many countries of the world simply the availability of adequate treatment) the risk of epilepsy associated deaths can be reduced.
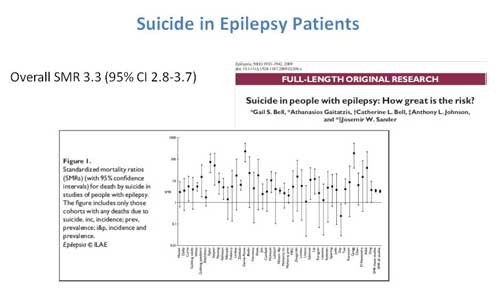
Figure 2. Risk for suicide among patients with epilepsy is greatly elevated in comparison to the general population. Summary of the standardized mortality rate in multiple studies.
The importance of treatment in reducing death rates has been emphasized by a number of studies. At present there are no data to determine whether more aggressive treatment of depression reduces suicide risk, but there is information regarding treatment and the risk of SUDEP. Dr Tomson reported several analyses of studies that indicated that medical non-compliance greatly increased the risk of SUDEP. He also presented data that suggested that monotherapy reduced the risk compared with no treatment, whereas being on three or more antiepileptic drugs increased the risk. Whether being on monotherapy indicated a less severe form of epilepsy with less risk or whether multiple medications increased the risk independent of disease severity will require further studies. In resource poor countries it has clearly been demonstrated that death rates decrease when people are on medications. The issue of effective treatment and SUDEP has also entered into the discussion for clinical trials, in which the mortality rate was much greater in the placebo arm and in the effective treatment arm (6.9 vs 0.9 deaths per 1000 patient years respectively). The issue of seizure control and SUDEP has also entered the surgical literature. Multiple studies have found that overall mortality as well as death from SUDEP was greatly reduced if patients were seizure free following surgery (Figure 3).

Figure 3. Epilepsy surgery reduces mortality from all causes, including SUDEP.
All studies suggest the value of stopping seizures in preventing deaths.
At the end of his presentation Professor Tomson made several important observations and suggestions. First, it is important to remember that preventable causes of death vary considerably from country to country, so that interventions to reduce epilepsy mortality will vary as well. In all cases minimizing seizure related accidents should be a health-care priority. Because seizure control significantly improves mortality rates, all efforts should be made to bring seizures, especially convulsive seizures, under control, either by medication or surgery. Finally, to reduce death rates, it is also important to address depression from which so many people with epilepsy suffer. The talk emphasized the importance of addressing the issues of safety as part of the treatment of epilepsy.
Subscribe to the ILAE Newsletter
To subscribe, please click on the button below.
Please send me information about ILAE activities and other
information of interest to the epilepsy community