Epigraph Vol. 17 Issue 1, 2015
Preventing Epilepsy After Injury

In recent years, one of the stated goals in the development of new treatments for epilepsy has been the prevention of the disease or modifying its underlying nature so that it has less impact on one's quality of life. Many researchers have tried to prevent the development of epilepsy after an injury or to lessen the severity of seizures that do develop. To date none of the approaches have resulted in strong or reproducible effects. In a presentation at the European Congress on Epileptology, Astrid Nehlig from Strasbourg reviewed the goals for antiepileptogenesis, what has been tried and what must be considered if epilepsy prevention is to become an achievable goal in the future.
As she noted, epileptogenesis is the series of changes that takes place in the brain after an injury that result in spontaneous seizures or that allows the progression of the epilepsy after the first seizures. Professor Nehlig pointed out that the process is complex with many steps and changes that we do not understand. In the current models of acquired epilepsy, it is not clear which changes may contribute to the development of epilepsy and which are a response to the injury and play no role in seizures.
It is possible that some changes could actually be working to prevent the development of epilepsy. The changes that occur after trauma, status epilepticus, and stroke include neuronal loss and changes in the blood brain barrier and in metabolism. There are certainly epigenetic processes that result in expression of different receptors and channels. Further there is glial activation and inflammation and rearrangement of neuronal circuits. She pointed out that with all of these changes in many regions it is difficult to know which of them are critical to epileptogenesis and which are irrelevant to it.
To date antiepileptogenic clinical and preclinical trials have not prevented epilepsy. Trials with a number of antiepileptic drugs or drugs which block activity at identified neurotransmitter receptors have not been successful. Various anti-inflammatory agents have been tried without major success. There have been attempts at gene therapy with various genes attached to virus as well as stem cell transplantation without significant benefit. Some studies have reported reduction in seizure frequency or the intensity of the behavioral seizures, but these results are difficult to interpret as in untreated animals there is great variation in outcomes.
Dr Nehlig pointed out that we do not know which molecular targets could play the critical role nor where we should direct treatment and when. The focus of efforts to date has been primarily the hippocampus in the models of limbic epilepsy, but there are other cortical and subcortical regions that may be just as important and should be targeted. Thus, failure to date may be from the failure to treat all of the contributing brain regions. Timing of treatment is also important. There is a cascade of events from the time of the injury to the first seizure and beyond, so it is likely that treatment targets will change over time. What may work at one time may have no effect at other times.
The problem is further compounded by the multiple causes and very distinct pathophysiologies across the different epilepsy types. As with many of the degenerative disorders there is a great need to identify mechanisms for which we can develop effective therapies. Epilepsy has the advantage in that our models have many parallels to the human disease, but perhaps the most important effort will be to focus on the changes that occur throughout the seizure generating regions during the development of epilepsy.
In her concluding remarks she suggested that our current efforts to prevent or ameliorate epilepsy are not likely to achieve the goal. However, Dr Nehlig did offer a path forward. It is most important to understand the changes that are involved in the development of epilepsy and when these changes occur. Because there are likely to be more than one and probably a number of mechanisms involved at different times in the evolution of the disease, we may ultimately need a combination of sequential treatments. At present, in view of our limited understanding of what is happening, any treatment will largely be based on speculation. In this situation, success will mostly be the result of pure chance. As we consider what should be targeted, Professor Nehlig emphasized the need to look at the whole epileptic circuit, and not just a single region such as the hippocampus. Further, because how the brain recovers may be influenced by factors in the environment, some attention should be given to the environment in which recovery occurs. She ended with the message that although we are not yet there, a careful evaluation of the many factors that contribute to epileptogenesis may get us there.
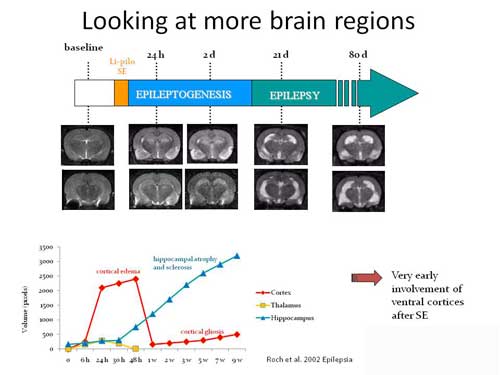
Figure 1: Time course of some of the changes that happen during the development of epilepsy after an episode of Status Epilepticus induced by lithium-pilocarpine. Top line shows the time line of epileptogenesis with the first spontaneous seizures beginning a week or more after the injury. The series of MRI scans demonstrates the evolution of changes with edema in the early phases after injury and the late development of atrophy. The graph plots the volume of the changes in edema and atrophy over time.

Figure 2: Injury of temporal cortices predicts development of epilepsy.
All of the young rats (21 days old) develop Status Epilepticus, but only those with injury develop epilepsy.
Subscribe to the ILAE Newsletter
To subscribe, please click on the button below.
Please send me information about ILAE activities and other
information of interest to the epilepsy community