Epigraph Vol. 24 Issue 4, Fall 2022
How can primary health care help to close the epilepsy treatment gap? A journey through Andhra Pradesh, India
Leer en español | Lire en français
By Nancy Volkers, ILAE communications officer
Cite this article: Volkers N. How can primary health care help to close the epilepsy treatment gap? A journey through Andhra Pradesh, India. Epigraph. 2022;24(4):73-77.
The role of primary health care in identifying, diagnosing, and treating people with epilepsy is increasingly important, particularly in view of the recent adoption of the Intersectoral Global Action Plan (IGAP) for Epilepsy and Neurological Disorders by the World Health Assembly.

However, societal attitudes and stigma around epilepsy can be major barriers to improving care. Without at least a rough idea of how many people require diagnosis and treatment in a given area, it’s difficult to establish needs and gaps. In India, where many people keep epilepsy hidden even from care providers, mapping the current state of epilepsy care in a rural area of Andhra Pradesh was nearly an exercise in futility.
A team of researchers visited two primary health care centers in Bhimaravam to assess care provided to people with epilepsy through the primary health care system. The visits were part of a coordinated clinical and research initiative called STOP-Epilepsy, which aims to improve epilepsy care in three districts in India:
- Gauriganj in Uttar Pradesh
- Bhimavaram in Andhra Pradesh
- Nawanshahr in Punjab
Bhimaravam, in coastal South India, has a population of about 225,000. Most people work in rice paddy cultivation or fish farming. The two health care centers—in Turputallu and Gollavanitippa—each provide service to approximately 50,000 people.
“Reaching the centers took us a few hours,” said Gagandeep Singh, an epilepsy researcher from India. “This was largely because navigating the pot-holed road was quite a challenge.”

At each center, the team interacted with medical officers, pharmacists, nurse midwives and Accredited Social Health Activists (ASHA) workers.
“We asked the medical officers how commonly they saw people with epilepsy during clinics,” said Singh. “At Turputallu, the doctor replied, ‘Not too many. I would see about 60 to 70 outpatients on any day and might see 1 or 2 people with epilepsy in a week.’”
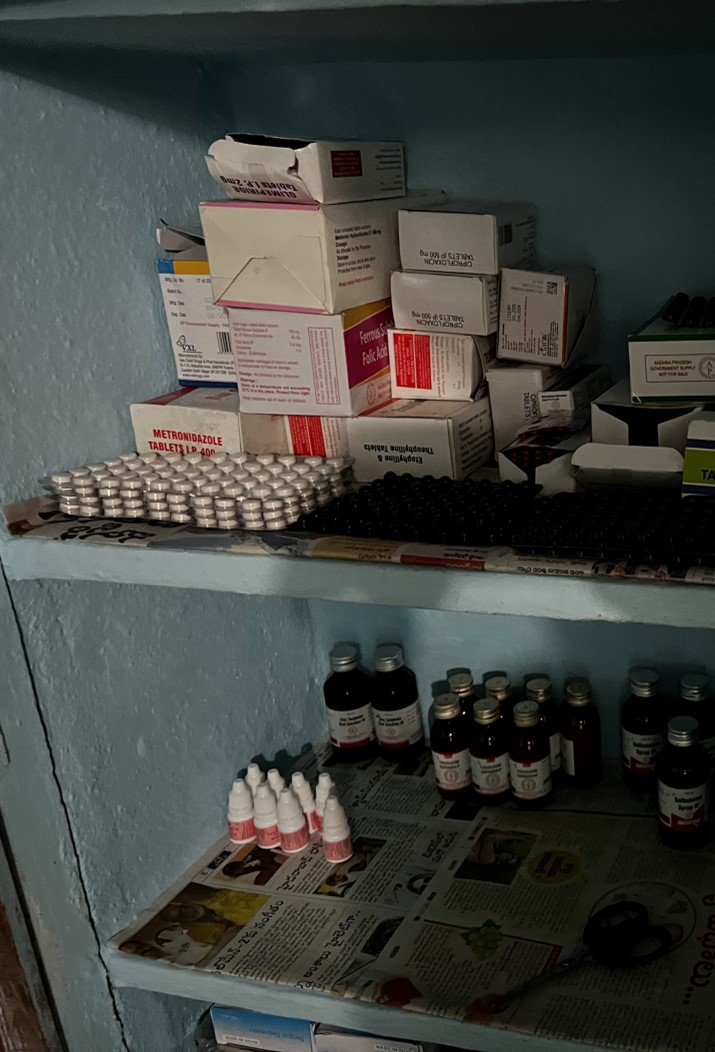
At Gollavanitippa, the pharmacist told the group that the pharmacy had 100 mg phenytoin tablets and injectable diazepam as anti-seizure medications.
“When we asked about other epilepsy medicines, he replied, ‘Other epilepsy medicines are never prescribed, and so we never requisition them,’” said Singh. The small numbers of people with epilepsy in the clinics was the main reason cited for the limited availability of anti-seizure medications.
|
ASHA workers in India: Community health at the village level Accredited Social Health Activist (ASHA) workers are female community members, usually between the ages of 25 and 40, who work mostly on a voluntary basis, though they do receive some financial compensation. They are trained by the Indian Ministry of Health and Family Welfare as part of the country’s National Health Mission, which aimed to establish one ASHA worker for every 1,000 residents ASHA workers must primarily be residents of the village or area they serve, and plan to remain living there for the foreseeable future. They promote healthy behaviors through education and prevention, assisting in health care access in villages and marginalized areas in Indian cities. They are a key factor in communication, awareness, and access to care in these areas. ASHA is not only an acronym; it means “hope” in Hindi. There are close to 1 million ASHA workers in India. In May 2022, ASHAs were one of six recipients of the World Health Organization’s Global Health Leaders Award. |
At Turputallu, the researchers asked ASHA workers how many people with epilepsy lived in the communities they served.
“There was a long silence,” said Singh, “after which one of the ASHA workers said she was aware of one such case in her village.”
When asked about problems that people with epilepsy could face, Singh mentioned that one worker believed people with epilepsy are usually fine but can have problems during “no-moon days.”
The idea that seizures are somehow affected by the moon’s phases has been around for thousands of years. Romans referred to people with epilepsy as “lunaticus” (moonstruck) and believed the gods intervened during certain phases. Limited research suggests a possible negative association between seizure frequency and the fraction of the moon illuminated at night; however, other research suggests an opposite trend.


At Gollavanitippa, ASHA workers at first said they knew of no one with epilepsy in their communities.

“As the interpreter persisted, one said that she knew of a family in her village in which both brother and sister both had epilepsy,” said Singh. “The sister died prematurely, and the brother is seeking treatment for epilepsy from a private facility. She also mentioned one woman who was on treatment and married off some time ago. But it seems that that the epilepsy was not declared during the marital negotiations, and there has been considerable discord between the natal and conjugal family on this account.”
Arranged marriages account for nearly 80% of all marriages in India and much of South Asia. Parents or elders in the family negotiate arranged marriages; potential marriage partners have little to no opportunity to meet or discuss issues.
In India, epilepsy was legitimate grounds for divorce until 1999, when the Hindu Marriage Act was amended to remove it, largely due to the efforts of neurologists. Despite the legal gains, societal beliefs about epilepsy remain negative.
“All ASHAs agreed that hiding epilepsy was fairly common among both genders, and this was done primarily by families to avoid ruining marital prospects,” Singh said. “Using indigenous medications or witchcraft was not common, however. People would like to visit a specialist, funds permitting.”

Singh said another ASHA worker recalled a man who had epilepsy. She thought he might be visiting a private practitioner but was taking his medication irregularly because he could not afford a consistent supply.
In regions of the world with few epilepsy specialists, the World Health Organization (WHO) encourages engagement of primary health care physicians and other health care providers in epilepsy care. However, said Singh, this visit suggested that at least in this Indian district, very few people with epilepsy visit primary health care centers. Even community health workers are aware of only a few people with epilepsy in the communities they serve.
“Where then do people with epilepsy seek care?” asked Singh. “There could be alternative pathways of care, but in the case of Bhimaravam, there is no use of alternative medicines or traditional healers. Do they merely remain behind shadows?”
Despite the number of anti-seizure medications on the WHO and Indian lists of essential medicines, primary health care dispensaries have few of these medications available. And primary care providers in Bhimaravam appear to see few people with epilepsy.
“Even if more people arrived at primary care centers for diagnosis and treatment of epilepsy, would care providers be able to manage their epilepsy effectively?” asked Singh.
The trip to Bhimavaram emphasizes that there are multiple barriers to obtaining effective care, he said.
“Cultural prejudices about epilepsy result in patients and families being unwilling to seek help for the condition or to tell health workers about the symptoms. Many community health workers don’t have the training to recognize seizures, to educate the community about epilepsy, or to recommend appropriate treatment in most cases,” he said.
“Finally, the availability of medicines at the community level is limited. Many of the standard epilepsy medicines are either not available at all or the availability is inconsistent. Reducing the treatment gap will require addressing all of these issues.”
|
Stigma as a barrier to research: Life experiences of women with epilepsy in India In 2014, Jane von Gaudecker conducted an intensive study of six women in Kerala, India, highlighting the issues they face surrounding marriage, as well as other psychosocial and medical issues. Von Gaudecker, currently assistant professor at Indiana University School of Nursing, dressed traditionally while conducting the study and spoke the local language fluently. However, she still came to be known as the “epilepsy lady,” which was a major barrier to interviewing women. Of the 21 potential participants, 8 of them would not speak with her, in spite of assured confidentiality, for fear that the community would associate them with epilepsy. They were afraid of the effects on their daily lives, as well as marriage prospects. Six women did agree to extensive interviews; the findings are detailed in a publication, as well as an Epigraph article. |
Subscribe to the ILAE Newsletter
To subscribe, please click on the button below.
Please send me information about ILAE activities and other
information of interest to the epilepsy community