Epigraph Vol. 24 Issue 4, Fall 2022
Inadequate first-line treatment for status epilepticus: The issue and solutions
Leer en español | Lire en français
By Nancy Volkers, ILAE communications officer
Cite this article: Volkers N. Inadequate first-line treatment for status epilepticus: the issue and solutions. Epigraph. 2022;24(4):56-60.
A benzodiazepine is the first-line treatment of choice for status epilepticus. Guidelines from the Neurocritical Care Society (2012) and the American Epilepsy Society (2016) recommend medication types, doses, and means of administration. However, recent studies have illuminated that benzodiazepines are not always given — and when they are, the dose is almost always too low.
Two recent analyses of data from the Established Status Epilepticus Treatment Trial (ESETT) found that less than one-third of patients received a first dose of benzodiazepines that met minimum guideline recommendations.
ESETT compared levetiracetam, fosphenytoin, and valproate as second-line treatments for status epilepticus. As part of the analysis, researchers reviewed the timing and dosing of first-line benzodiazepines received by study participants.
Most doses too low
First-line treatment was not part of the ESETT protocol; it was administered according to local standards of care by caregivers, emergency responders, or emergency department personnel. However, best practices based on the AES guidelines were part of study training.
As a part of an interim analysis for ESETT, trial investigators also reviewed preliminary benzodiazepine dosing data. That analysis – published in 2019 – found that only 29.8% of first doses met the AES guideline recommendations.
ESETT investigators re-emphasized the guidelines and their evidence base with participating sites and provided supplemental training and education. A found that the intervention had no significant effect: Among all first doses given to ESETT participants, 32.4% met the minimum recommendations.
Guidelines recommend one or two doses of first-line treatment, depending upon the chosen medication. ESETT participants received multiple smaller doses of benzodiazepines—as many as nine, with most receiving two or three. Despite the multiple doses, 17% of people receiving first-line treatment never received a cumulative adequate dose.
Too little, too late

“As status progresses, it gets harder to treat,” said Abhishek Sathe, first author of the 2019 and 2021 publications and currently a senior clinical pharmacologist at Gilead Sciences. “Most adults received the equivalent of 2 mg of lorazepam – that’s basically half the dose. Then they got another half dose later, when the seizure did not stop. There may have been 4 mg given in total, but it was not given as a full dose, as the guidelines state — and that may be one of the reasons why these individuals continued to remain in status.”
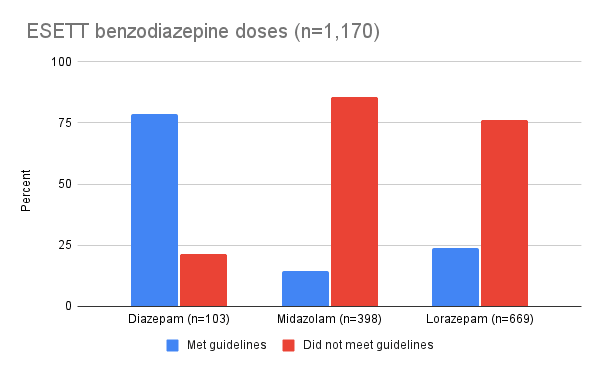
The ESETT analyses revealed distinct patterns for the first dose of each benzodiazepine option:
- Diazepam: 85.9% of first doses met guidelines. Diazepam was most commonly given by caregivers; 71% of diazepam administrations were given prior to the arrival of emergency services.
- Midazolam: 18.9% of first doses met guidelines. Two-thirds of midazolam doses were given by emergency medical services personnel, before hospital arrival.
- Lorazepam: 24.1% of first doses met guidelines. Nearly all lorazepam doses (91%) were given in the emergency department.
“What surprised me was that the home treatments, by family members, met the guidelines in most cases, whereas trained health professionals opted to use lower-than-recommended doses,” said James Cloyd, PharmD, senior author of the 2019 and 2021 publications, who noted that treatments for home use have fixed doses and are relatively straightforward to administer.
| Benzodiazepine |
% receiving recommended first dose Weight > maximum dose |
% receiving recommended first dose Weight < maximum dose |
% receiving at least 80% of recommended first dose All weights combined |
|---|---|---|---|
| Diazepam | 41.6% | 93.9% | 89% |
| Midazolam | 17.9% | 20.3% | 23% |
| Lorazepam | 13.3% | 46.0% | 33% |
ESETT is not the first analysis to find persistent benzodiazepine underdosing in the treatment of status epilepticus. Other studies have shown similar patterns; some have found associations between inadequate benzodiazepine treatment and progression to refractory status epilepticus, as well as worse clinical outcome overall.
Some studies find no association between adequate benzodiazepine dose and clinical outcome, though other variables — such as etiology, time to first-line treatment, and time to second-line treatment — play significant roles in outcome as well.
Why does underdosing persist?
“There has always been a concern that benzodiazepines can be harmful. The guidelines state clearly to administer a full dose using the correct route of administration, and in some cases an additional dose. There is evidence that this is not a safety concern,” said Cloyd. Cloyd is a professor in the University of Minnesota’s Department of Experimental and Clinical Pharmacology, as well as director of the University’s Center for Orphan Drug Research.

Concern about respiratory depression may drive some of the low dosing patterns, said Sathe. However, research has not shown that the guideline-recommended doses of benzodiazepines are associated with increased respiratory issues in status epilepticus patients.
“Status epilepticus itself can lead to respiratory depression,” he said. “The guidelines state clearly to administer a full dose using the correct route of administration, and in some cases an additional dose. There is evidence that this is not a safety concern.”
Evidence includes a 2001 study comparing diazepam, lorazepam, and placebo for prehospital treatment of status epilepticus. The study found similar rates of respiratory and circulatory complications among the three groups, with the placebo group trending higher (10.3% diazepam, 10.6% lorazepam, 22.5% placebo, p=0.08).
A 2020 study of midazolam for prehospital treatment of status epilepticus in adults found that although no patient received a guideline-recommended dose, higher doses were not associated with increased risk of respiratory issues. In fact, higher doses were associated with a slight reduction in the risk of needing respiratory support (OR 0.9; 95% CI 0.8-1.0).
Guideline awareness

Cloyd said that the gap between guideline release and clinical uptake is not surprising, given that it can take up to 10 years for a guideline to be implemented. “Guidelines are good, but you need to widely publicize them if you want to see an uptick in use,” he said. “Professional education through grand rounds, medical societies, [emergency medical services] (EMS) agencies, ER nurses.”
A 2019 JAMA study in California found that only 2 of 33 EMS systems followed evidence-based guidelines for status epilepticus treatment, though 17 of the 33 had revised their protocols after the publication of the AES guidelines in 2016.
Midazolam was the preferred treatment in the California EMS protocols, and intramuscular midazolam was included in 32 protocols. However, only 2 provided the correct dose recommendations; the others provided lower doses. Sixteen protocols also included intraosseous midazolam as an option, possibly due to older published pediatric recommendations.
“EMS protocols need to be updated and aligned with guidelines,” said Sathe. “Refresher training for EMS personnel might also be helpful.”
Collaboration
A commentary by Nicolas Gaspard reviewed a 2020 study of records from one EMS agency in the United States. The study analyzed all adult patients treated for status epilepticus over a five-year period (January 2013 to January 2018). Midazolam was the only available benzodiazepine.

Among 2,494 cases, 38% received no midazolam. Of the 62% that received midazolam, none received the correct dose. Intranasal (47.0%) and intravenous (38.3%) were the most common routes of administration, with 14% receiving the drug intramuscular (as recommended in the guidelines) and 1% receiving intraosseous injection.
Gaspard wrote, “We, as neurologists and epileptologists, are rarely directly involved in the management of early status epilepticus. But it should be among our priorities to disseminate the available evidence, and to collaborate with EMS agencies, emergency and critical care physicians to develop and implement local protocols based on national and international guidelines, as well as quality improvement programs. Evidence and guidelines themselves will not be sufficient.”
A hospital-EMS partnership
Researchers at Seattle Children’s Hospital (USA) are working with EMS agencies to improve the accuracy of pediatric weight-based dosing in emergent situations. Clinicians and EMS medical directors collaborated on the creation of Medic One Pediatric (MOPed) length-based color-coded dosage cards, which are based on Broselow tape length ranges.

“The initial intervention of the standardized dosing card was created for the most frequent EMS-encountered pediatric diagnoses,” said Lindsey Morgan, the study’s senior author. “The focus was on decreasing cognitive load for EMS personnel and increasing speed and accuracy for medication administration.”
EMS personnel were trained in how to use the MOPed cards; in a follow-up survey, 97% reported that the cards were their primary reference for pediatric dose calculations.
A 2022 analysis in Pediatric Neurology found that the MOPed cards and training increased accurate benzodiazepine dosing from 48% in the year before implementation to 94% in the year after.
Since the study’s publication, other quality improvement measures are underway, said first author Jennifer Keene. “Levetiracetam has been made available to EMS teams in the county, and we are continuing to work on improving communication to streamline the care of children as they transition from EMS care to the emergency department,” she said.
Subscribe to the ILAE Newsletter
To subscribe, please click on the button below.
Please send me information about ILAE activities and other
information of interest to the epilepsy community